
Patient age: 37 years • Female
Case Narrative
A 37-year-old female presented with pelvic discomfort including dyspareunia and lower-extremity
fatigue/heaviness, particularly after prolonged standing.
Given concern for iliac venous outflow obstruction with pelvic venous congestion physiology, she
underwent intravascular ultrasound (IVUS) evaluation of the left common iliac vein (L-CIV). IVUS
planimetry demonstrated a severe focal L-CIV stenosis with reference cross-sectional area (CSA)
159.4 mm² and minimal CSA 41.3 mm², corresponding to an approximate 74% area reduction (Fig 1).
The IVUS analysis summary documented approximately 74% area reduction and 93% blood-flow
reduction at the test site (Fig 2), consistent with hemodynamically significant iliac obstruction and
correlating with her pelvic symptom complex.
She subsequently underwent iliac venography/fluoroscopy-guided intervention. Initial pelvic imaging
documented baseline catheter positioning and pre-treatment appearance (Fig 3). The lesion was
crossed and treated in standard stepwise fashion with working views confirming positioning for
intervention (Fig 4), followed by angioplasty across the stenotic segment (Fig 5-6).
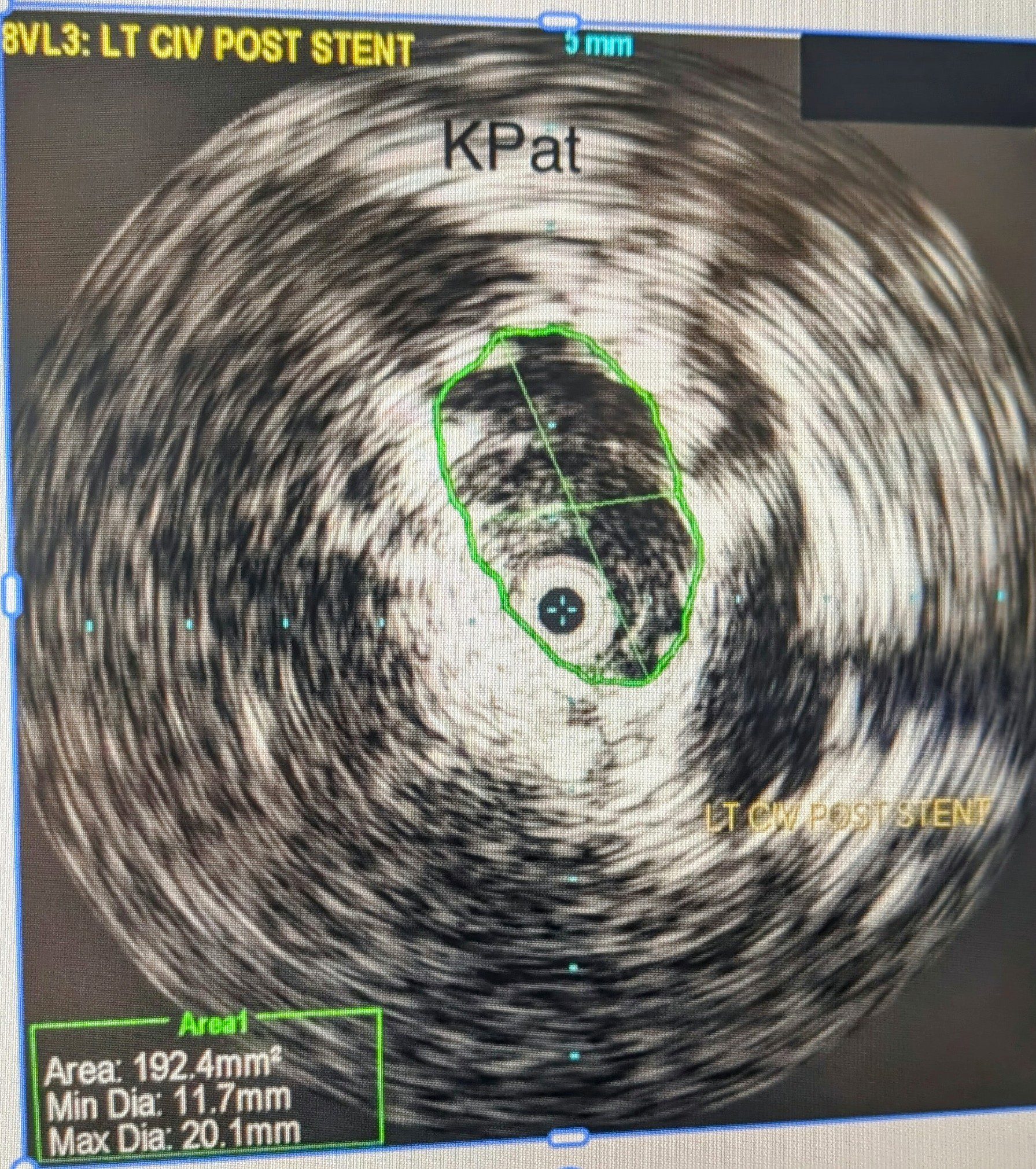
Completion imaging demonstrated the deployed iliac venous stent framework with restoration of inline
outflow (Fig 7). Post-stent IVUS confirmed a markedly expanded lumen with post-stent CSA 192.4 mm²
min diameter 11.7 mm, max diameter 20.1 mm), supporting an excellent technical result (Fig 8). The IVUS
summary screen reported substantial post-intervention improvement metrics (Fig 2).
At 1-month follow-up, the patient reported overall clinical improvement, including improved dyspareunia
and improved leg fatigue/heaviness with prolonged standing, consistent with clinical success in addition
to documented radiographic/IVUS success.
She remained on therapeutic anticoagulation post-procedure, with a brief interruption of approximately 2 days
during menses due to heavy menstrual bleeding, after which anticoagulation was resumed and planned to
continue for the next couple of months per protocol.
She noted persistent dysmenorrhea during her first post-stent menstrual cycle, with counseling that pelvic venous
congestion symptoms may continue to improve over subsequent months as pelvic collateral burden diminishes.
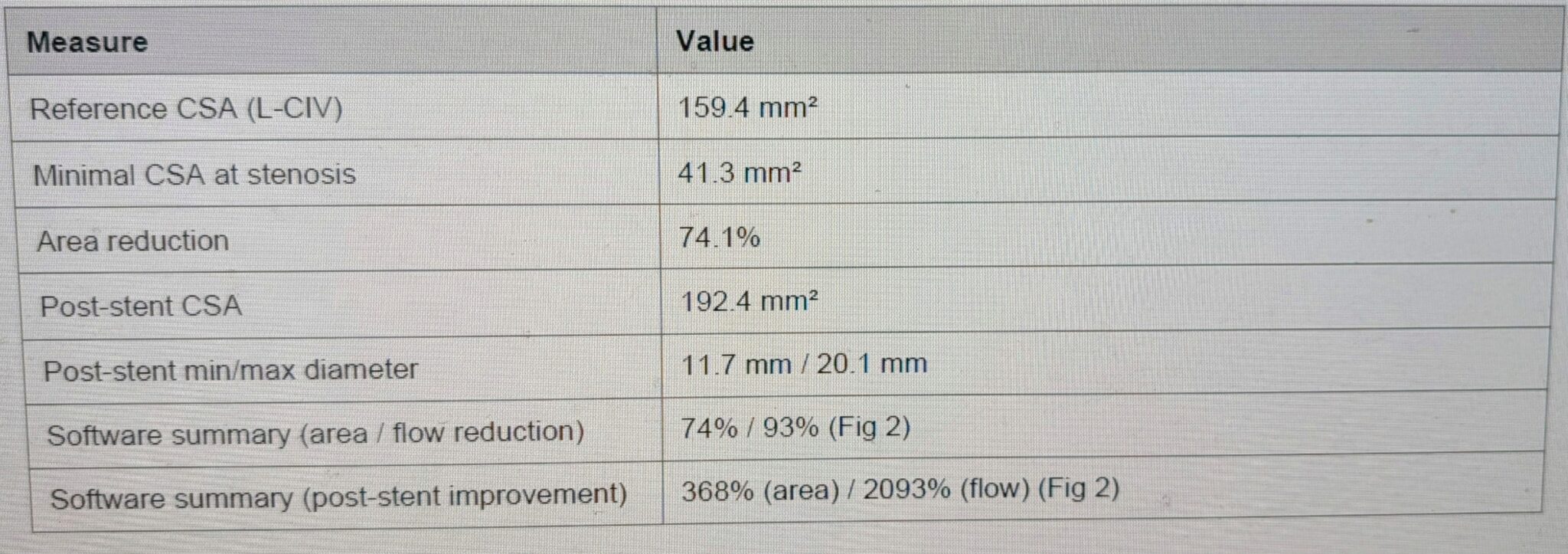
Key Quantitative Findings
Call Or Request An Appointment
Contact us to schedule an appointment with our expert Vein Specialists team. We will evaluate your signs and symptoms, answer your questions, and create a personalized vein care treatment plan to relieve your leg pain and enhance your life.
Schedule Your Appointment TodayFigure 1. Pre-stent IVUS – L-CIV stenosis (LT CIV DIFF).
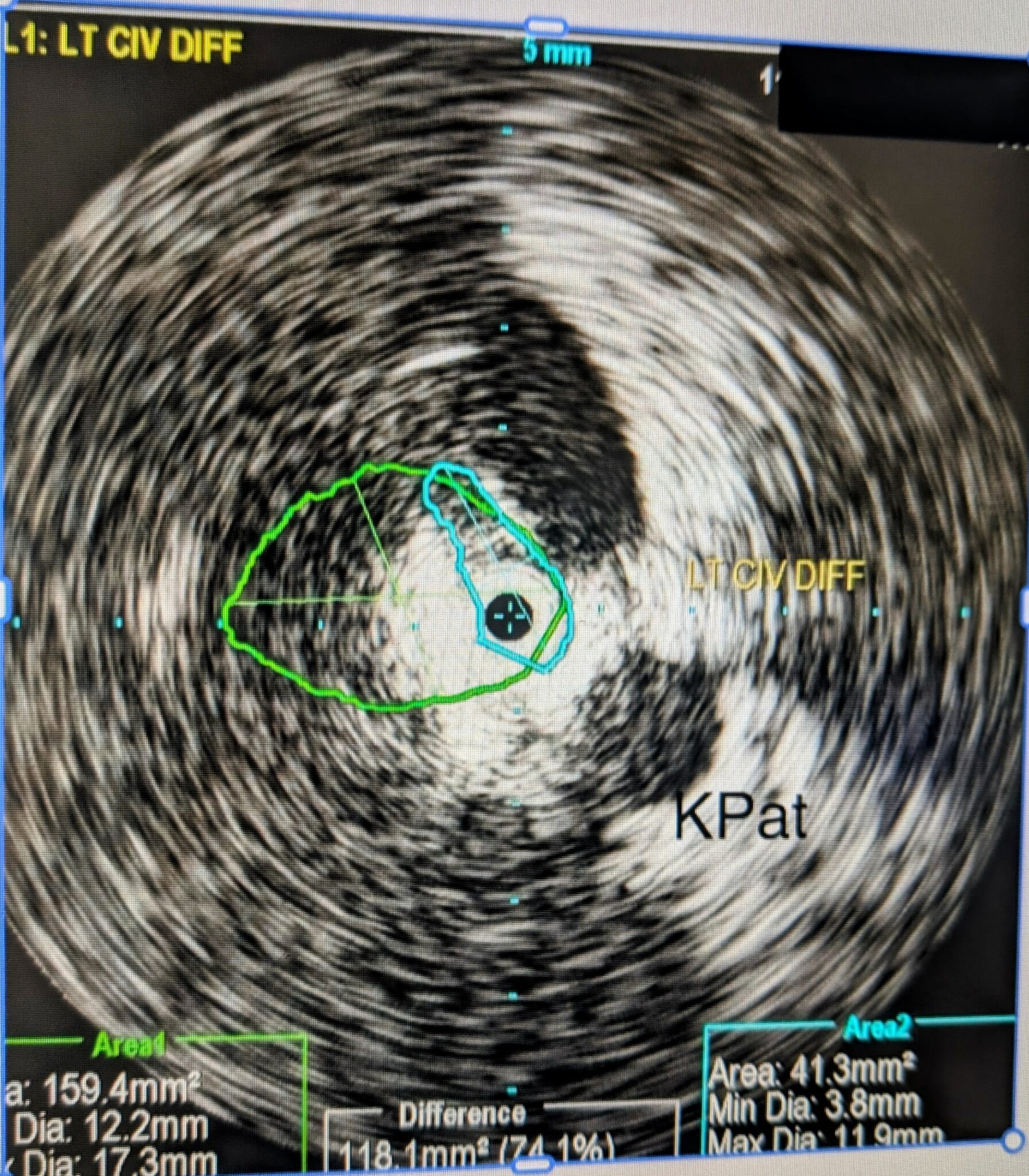
Figure 2. IVUS Data Analysis summary – L-CIV.
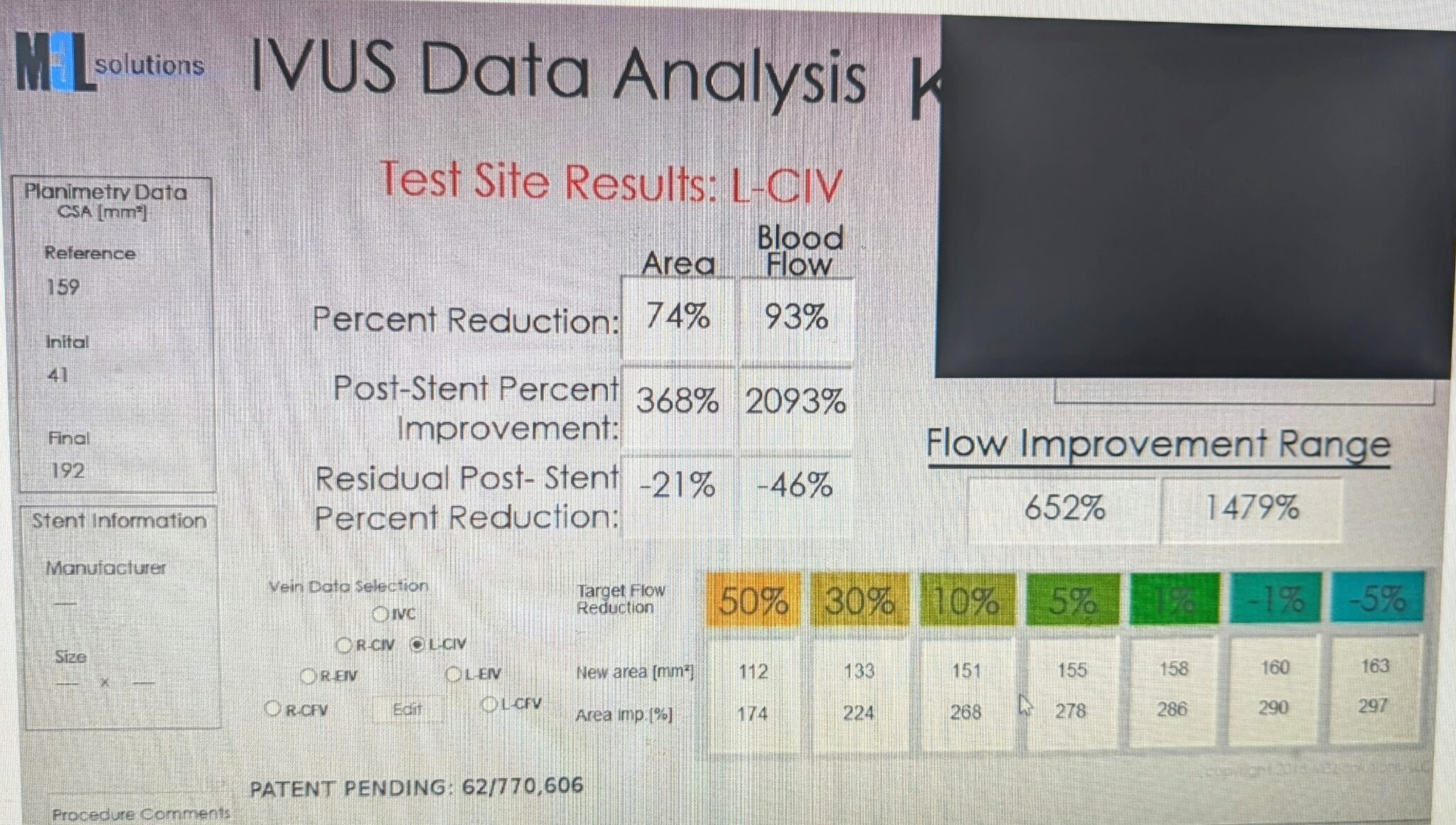
Figure 3. Pelvic fluoroscopy – KP1 (baseline view).
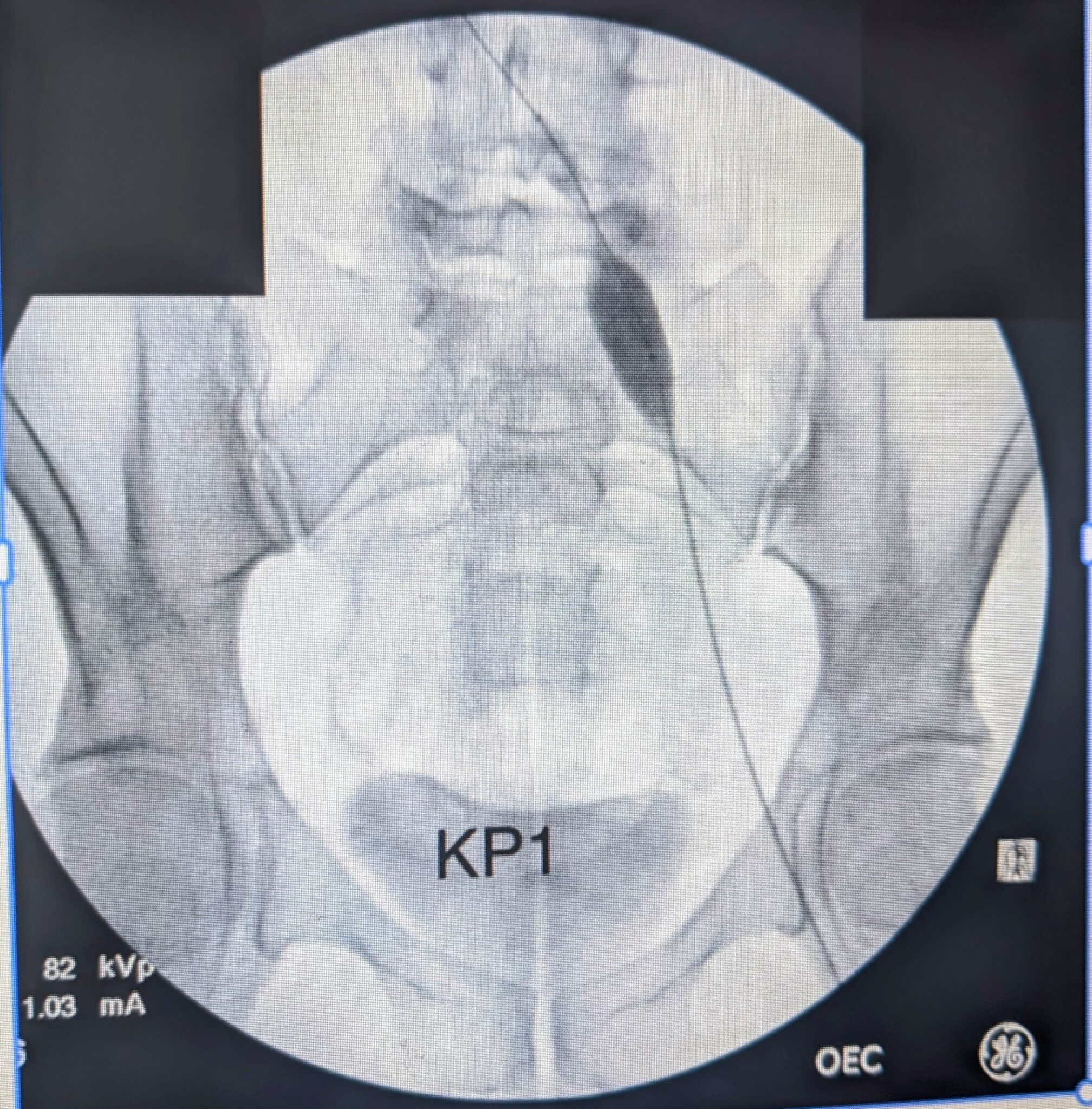
Figure 4. Pelvic fluoroscopy – KP2 (working view).
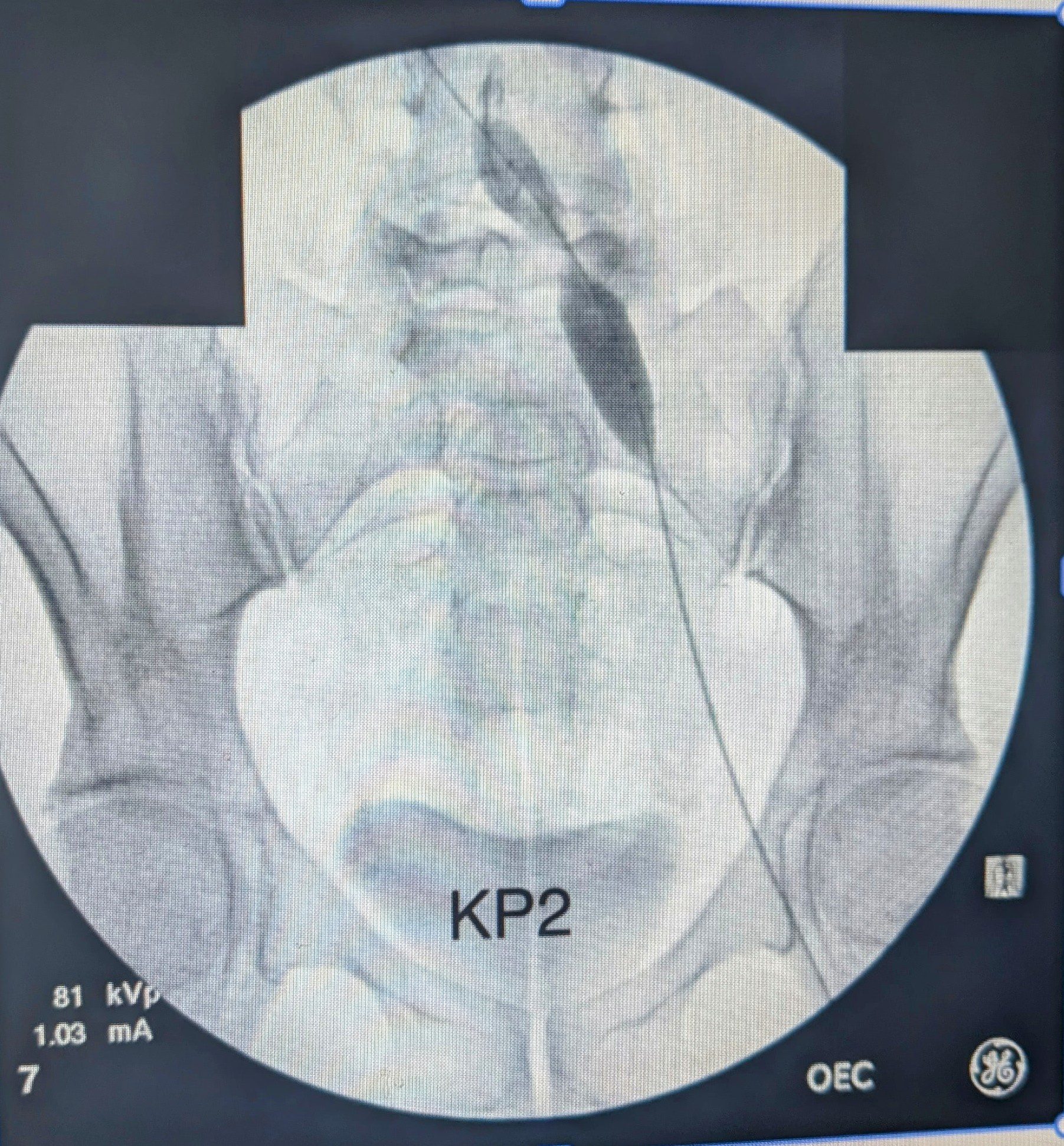
Figure 5. Pelvic fluoroscopy – KP3 (angioplasty step).
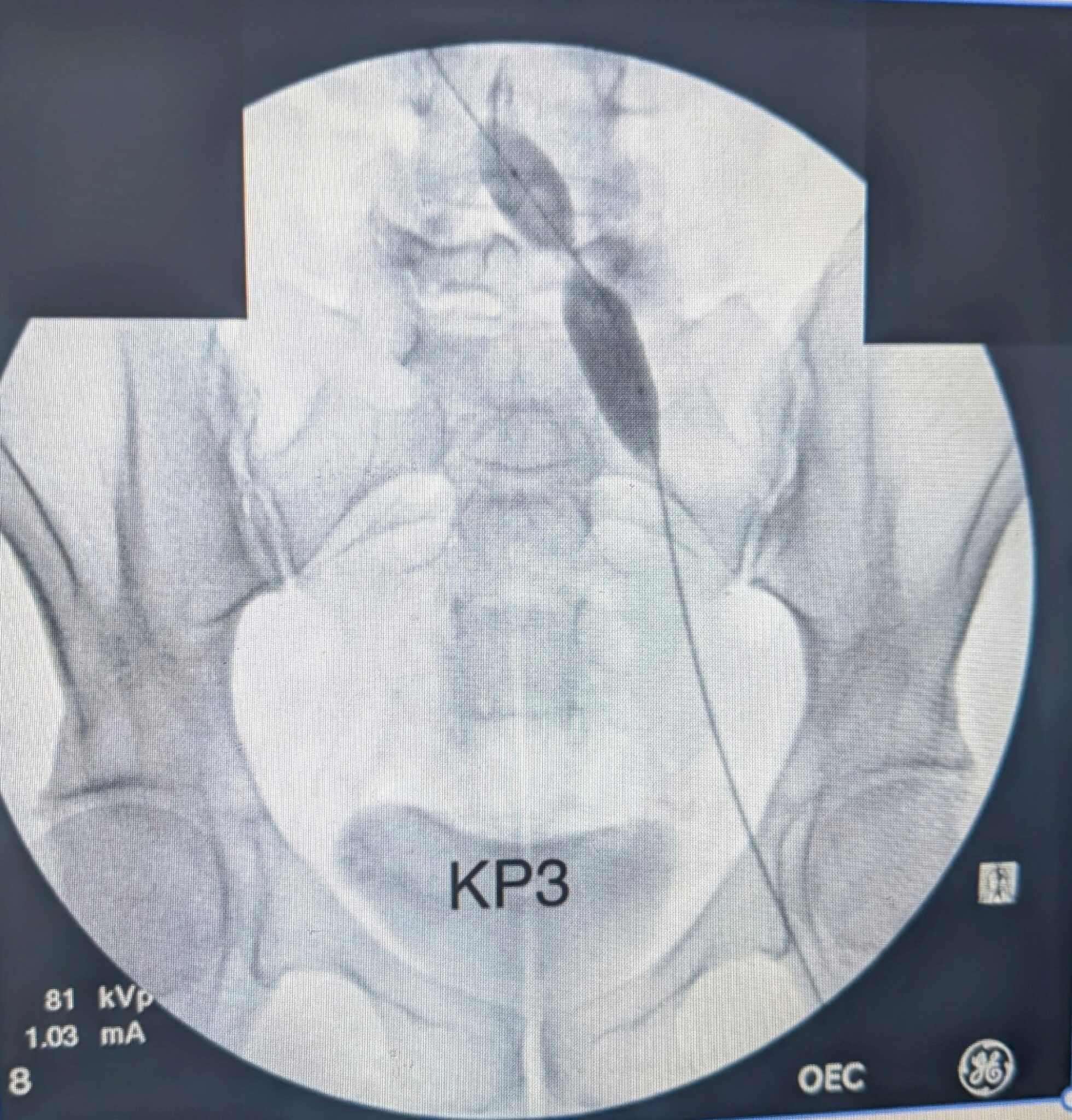
Figure 6. Pelvic fluoroscopy – KP4 (angioplasty/sizing step).

Figure 7. Pelvic fluoroscopy – KP5 (post-stent appearance).
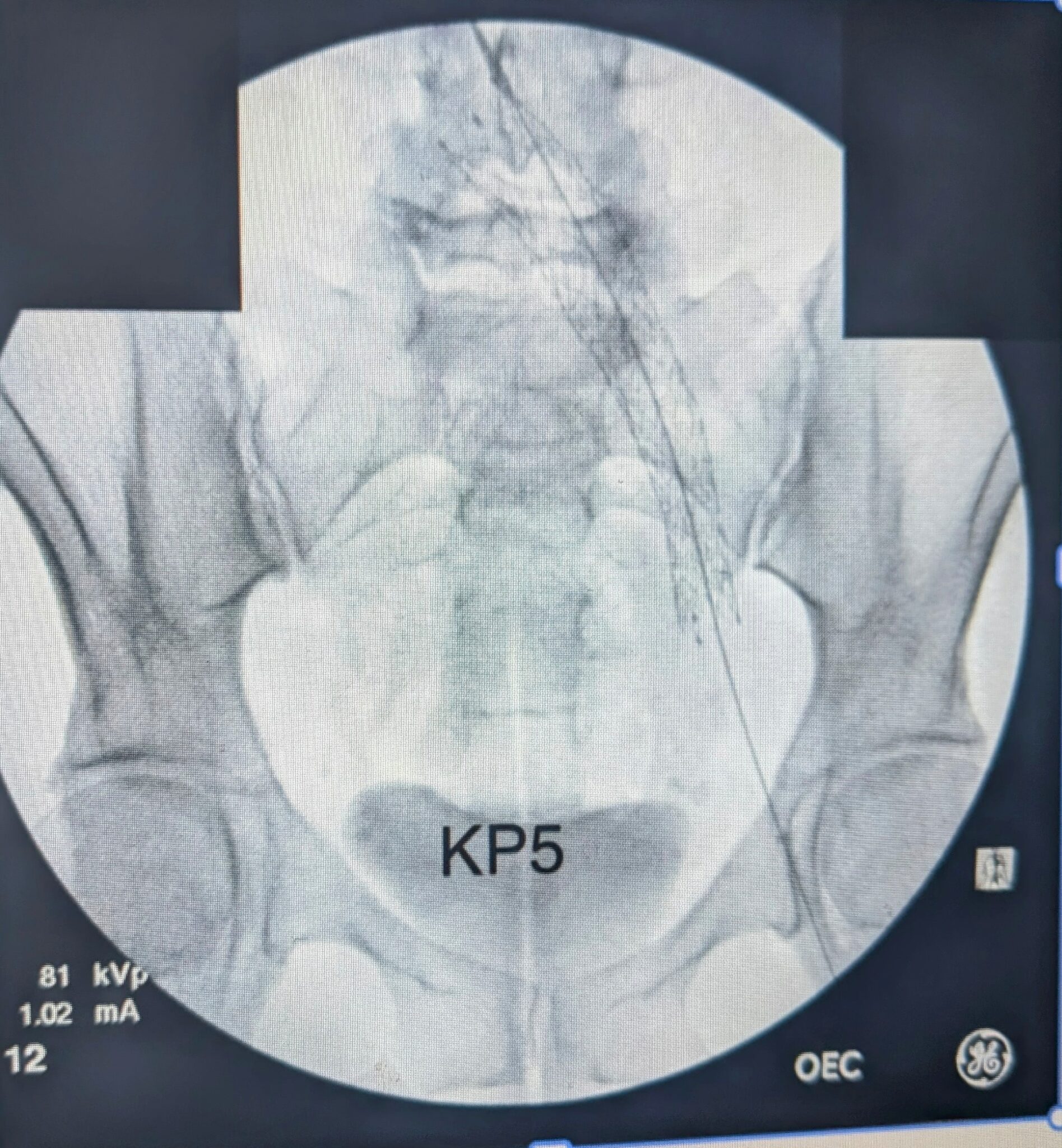
Figure 8. Post-stent IVUS – L-CIV (LT CIV POST STENT).
Request an Appointment
Please take a moment and fill out your request below and one of our staff members will be in contact within 24-48 business hours. If this is an emergency, call 911 immediately. If this is a non-emergent concern, please call the office Monday-Friday between 8am – 5pm at: 239-694-8346
